
Treating a receding hairline is different from treating crown thinning. The hairline is harder. Products that work well on the vertex often deliver weaker results at the temples. Understanding why, and choosing accordingly, is the difference between wasted time and actual progress.
Why the Hairline Is Harder Than the Crown
Three factors make frontal hairline treatment more challenging:
- Higher androgen receptor density. Temple follicles have more androgen receptors per follicle than crown follicles in most men. They are more sensitive to DHT and miniaturize faster.
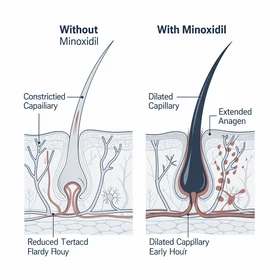
- Lower blood supply. The temporal region has less robust blood circulation than the vertex. Treatments that rely on improved blood flow (minoxidil) are less effective here.
- Earlier miniaturization. By the time most men notice hairline recession, those follicles have been miniaturizing longer than crown follicles. There is less viable tissue to work with.
This is why clinical trials consistently show better outcomes at the crown than the hairline across every treatment category. It does not mean the hairline is untreatable. It means your expectations and product selection need to account for this reality.
Treatment Rankings for Hairline Specifically
1. DHT Blockers (Best for Hairline Prevention)
Since the hairline's primary vulnerability is DHT sensitivity, blocking DHT is the most logical first-line approach for hairline recession specifically. DHT blockers address the cause rather than compensating for the symptom.
Finasteride: The strongest single-agent option for halting hairline recession. Clinical data shows it is more effective at preventing further recession than at regrowing lost hairline. This is key: start early, when the goal is preservation.
Natural DHT blockers (Procerin, saw palmetto): Lower potency, but still addresses the right mechanism. Best for early-stage recession (Norwood I-II) where the goal is to slow progression while follicles are still viable. For a comprehensive look at how DHT specifically drives hairline recession, recedinghairline.org covers the mechanism in depth.
2. Finasteride + Minoxidil Combination
The combination addresses both the cause (DHT) and the growth stimulation pathway simultaneously. Published data shows 94% improvement rate with combination therapy. For men at Norwood III or higher, this is the most evidence-backed medical approach.
Apply minoxidil specifically along the hairline edge. Some men find the foam formulation easier for targeted temple application than the liquid.
3. Minoxidil Alone (Weaker for Hairline)
Minoxidil's clinical data is strongest for the crown. At the hairline, results are less predictable. That said, some men do respond at the temples, particularly when using the 5% foam formulation with consistent twice-daily application directly to the recession area.
Use minoxidil at the hairline as an adjunct to a DHT blocker, not as your sole intervention.
4. Microneedling + Topical Treatment
Dermarolling (0.5-1.5mm depth) at the hairline before applying minoxidil or a topical activator increases absorption and may stimulate dormant follicles through wound-healing growth factor release. Early clinical data is promising for hairline-specific improvement, though larger studies are needed.
5. Hair Transplant (For Established Recession)
For men at Norwood III+ with stable recession who want to restore the hairline, FUE transplant is the only option that physically adds hair to bald areas. Modern techniques produce natural-looking results. Requires ongoing DHT management post-surgery to protect surrounding native hair.
Step-by-Step Approach for Hairline Treatment
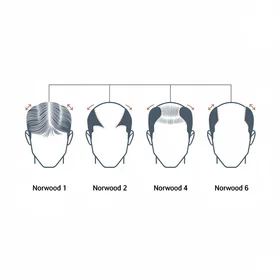
- Confirm your stage. Take photos, compare to the Norwood scale. Be honest about whether you are at II, III, or beyond.
- Start a DHT blocker immediately. Whether natural (Procerin for low-risk start) or prescription (finasteride for maximum effect), blocking DHT is the foundation. Every month of delay is follicles lost.
- Add minoxidil at the temples. Apply foam directly to the hairline recession area twice daily. Give it 6 months before evaluating.
- Consider microneedling. A 0.5-1.0mm dermaroller used weekly at the hairline before topical application. Clean technique is essential.
- Evaluate at 6 months. Compare photos. If progression has slowed or stopped, continue. If not, escalate to prescription strength or combination therapy.
- Transplant consultation at 12+ months. If your hairline is stable on treatment but you want restoration of already-lost territory, consult a reputable FUE surgeon. Only after 12+ months of stability to ensure the surgeon is working with a predictable baseline.
What Results Actually Look Like
Realistic hairline treatment outcomes at 12 months:
- Best case (early intervention, combination therapy): Recession halted, minor thickening at temples, some baby hairs at the hairline edge filling in
- Typical case (moderate recession, DHT blocker): Progression stopped, existing hair maintained, no further deepening of temple points
- Limited case (advanced recession, late start): Slowed progression, some stabilization, but no restoration of lost hairline territory
Notice that none of these include "full restoration to juvenile hairline." That is not a realistic outcome from any non-surgical treatment. The goal is stopping the bleed and potentially recovering some ground at the edges. For a look at how the DHT mechanism specifically targets the hairline first, dhthairloss.info explains the biology behind why temples are ground zero.